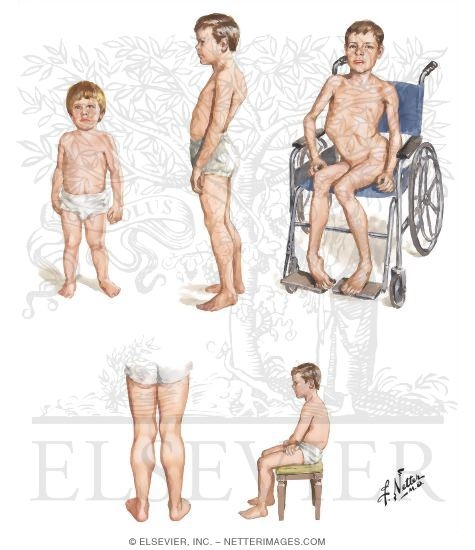
Muscular dystrophies are genetically determined diseases characterized by progressive deterioration of skeletal muscle function without affecting peripheral nerves or the system CNS. Duchenne muscular dystrophy, in particular, is an autosomal recessive myopathy linked to chromosome X, whose pathophysiological basis is the absence of dystrophin in the sarcolemma. Dystrophin is responsible for maintaining the integrity of the muscle membrane. The lack of this protein or its dysfunction leads to instability of the membrane, a progressive leakage of intracellular components and an elevated CPK. This happens not only in skeletal muscle and smooth, but in the heart muscle and brain. In the end, the cell units with impaired dystrophin are captured by macrophages and destroyed cells are replaced destruidas.Las by fibrofatty infiltration leading to proximal muscle weakness and pseudohypertrophy in joints and muscles affected to a lesser extent, muscle cardíaco.En it, the replacement of myocardium by fatty tissue results in dilated cardiomyopathy. The demonstrations in the electrocardiogram is sinus tachycardia, tall R waves in right precordial leads, prominent Q waves in left precordial leads and inverted T waves due to scarring of the left ventricle. With progression of the picture, may be ventricular arrhythmias and CHF. ACE inhibitors are preferred in the early stages and can use beta blockers. From the point of Respiratory view, these patients developed progressive fatigue and exhaustion of respiratory muscles, which does not help a restrictive pattern, with difficulty in expelling secretions, conditioned by deformities of the rib cage.
Well, those patients whose life expectancy is 15-25 years extend to the operating room and their anesthesiologists, we need to know a set of guidelines to avoid complications.
preanesthesia:
- CXR: for deformities of the chest and possible tracheobronchial compression.
- Arterial blood gas can be hypercapnic hypoventilation.
- Lung function tests: there is a decrease in the CV and the CPT.
- ECG: with the changes outlined above.
- echocardiography ejection fraction: To assess the degree of myopathy and the presence of valvular heart disease (10-20% of patients have a mitral valve).
- If necessary: \u200b\u200bHolter.
- Assess swallowing disorders also malnourished or gastrostomy.
- Possible sleep apnea may contribute to pulmonary hypertension. Intraoperative
: Dantrolene Check stock in the hospital
- There may be a decrease in laryngeal reflexes and increased gastric emptying time, increasing the risk of aspiration
- Difficult airway by deformities and muscle contractures as well as the difficulty of placement.
- Contraindicated succinylcholine and halogenated due to the possibility of severe hyperkalemia and rhabdomyolysis due to the instability of the sarcolemma.
- Increased sensitivity to nondepolarizing muscle relaxants .
- can be used opiates, but we recommend short-acting and small increments doses.
- Increased risk of arrhythmias . Postoperative
:
- Increased risk of respiratory failure and respiratory infections, with difficulty for the withdrawal of mechanical ventilation for respiratory depression secondary to anesthetic drugs and prolonged paralysis.
- Chest physiotherapy
-
early nutritional support - Poor wound healing, thus, higher incidence of suture dehiscence.
If you want to know more about the issue, the journal Chest in its December issue in 2007 he published an article of consensus on the anesthetic management of patients with Duchenne ( American College of Chest Physicians Consensus Statement on the Respiratory and Related Management of Patients With Duchenne Muscular Dystrophy Undergoing Anesthesia or Sedation ).

0 comments:
Post a Comment